Do Tadalafil/Sildenafil Illicit Hypertrophic Responses?
Tadalafil is a potent phosphodiesterase-5 inhibitor (PDE5i) that is commonly prescribed for erectile dysfunction [1] under the brand name Cialis. Due to it's effects on skeletal muscle vasodilation, many bodybuilders use tadalafil to enhance the blood flow to their muscles during a training session (known as "the pump"). Interestingly enough, tadalafil not only increases blood flow transiently, but it may also positively influences hypertrophy through mechanisms I will explain in this article.

Mechanism of Action
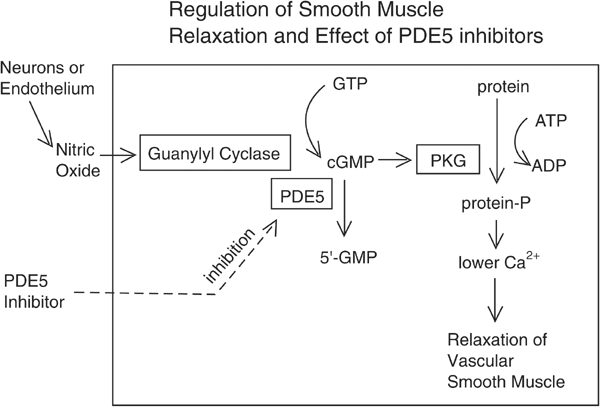
To understand how tadalafil may increase hypertrophy, you must first understand the basics of how it works biologically. Tadalafil, as mentioned earlier, inhibits an enzyme known as phosphodiesterase-5. This enzyme is responsible for breaking down cyclic guanosine monophosphate (cGMP), a nucleotide responsible for carrying out actions of vasodilation in response to nitric oxide. So, technically, tadalafil does not give you the "pump" directly, but rather through decreasing the breakdown of the chemical that gives you the "pump".
This might seem like a lot of information to take in, but it will be helpful later in understanding some of these studies.
Point 1 - Sildenafil increases MPS in vivo
As we all should know, human in vivo data is the most applicable to us and thus should be used as the most valid type of data over human in vitro data, data collected from other species, and data/hyoptheses extrapolated from biochemical mechanisms.
Though there is not much human data in vivo (occurring in the whole organism - not just cells in a petri dish) on PDE5 inhibitor's effects on muscle protein synthesis (MPS), there is one study in particular that we can look at. In this study [2], 12 subjects were either given 25mg of sildenafil (n=6), or a placebo (n=5) for 15 days.
Researchers observed two changes:
- MPS in the sildenafil group was double that of the placebo group
- Muscle fatigue was significantly lower in the sildenafil group (subjects given sildenafil were able to perform more repetitions of a selected exercise)
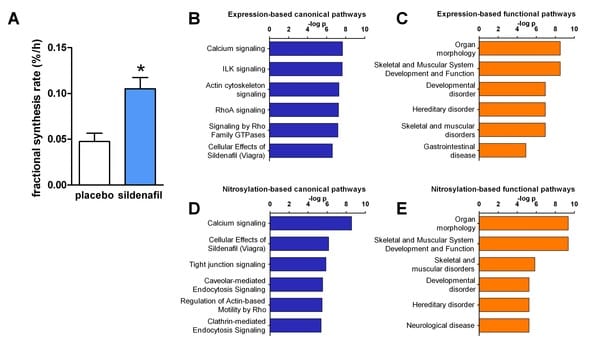
The authors of this study described the increase in MPS response as, "of similar magnitude to that observed in response to 100–200 mg/week testosterone injection".
Does this mean conclusively that sildenafil and other PDE5 inhibitors absolutely cause muscle gain? Not necessarily, but it's a great starting point. The only issue I have with this study is it's extremely small sample size.
Point 2 - PDE5i's reduce muscle weakness in dystrophic rodent muscles
Duchenne muscular dystrophy (DMD) is a disease characterized by a restriction of blood flow to the muscles, and as a result, a breakdown of skeletal muscle. In multiple studies [3, 4], PDE5 inhibitors have been shown to reverse or mitigate the effects of DMD (mdx) in rodents.
In one study [3], mdx mice (rodent equivalent of DMD) showed a reversal of skeletal muscle breakdown following tadalafil administration. Although one could argue that tadalafil is simply reversing the ischemia (blood flow reduction) in the mice and returning their muscles back to baseline, reading deeper would show that this isn't necessarily the case. The researchers induced similar ischemia in the control mice (non-mdx), and they found that ischemia alone was not enough to cause muscular breakdown. So why would tadalafil reverse this damage, if it is not solely blood flow?
Researchers explained this by hypothesizing that DMD has a "two-hit mechanism", in which blood flow is only one portion of the disease. They found that not only is blood flow reduced in the mdx mice, but also nitric oxide (NO) signaling. This very well could be the second contributing factor in DMD, as NO is somewhat responsible for regulating muscular regulatory mechanisms (this will be discussed further in the next section). It would also explain why tadalafil reverses the dystrophic symptoms of the mdx mice, as it increases NO signaling through elevating cGMP.
Again - this is absolutely not conclusive evidence on it's own to show that tadalafil and other PDE5 inhibitors increase hypertrophy. As we start to add to our list of evidence, though, the hypothesis of tadalafil increasing hypertrophy becomes more and more plausible.
Point 3 - Hypothetical Mechanisms
We see from the aforementioned data that tadalafil may plausibly increase hypertrophy, but we then must explore if it makes sense logically by exploring the biological mechanisms. Since tadalafil inhibits the breakdown of cGMP and elevates NO signaling, we can extrapolate the skeletal muscle-related effects that tadalafil may have by observing data from the documented role that cGMP and NO play in skeletal muscle regulation.
According to two studies in particular [5, 6], increases in activation of cGMP via elevating NO induce mitochondrial biogenesis. Authors in both studies have made it clear that this effect is mediated through cGMP rather than NO itself. This piece of information may exhibit one mechanism by which tadalafil may increase hypertrophy - by increasing mitochondrial biogenesis indirectly. Since the mitochondria generates most of the chemical energy needed to facilitate biochemical reactions, this would make sense in theory.
According to multiple studies [7], increases in skeletal muscle via resistance training are accompanied by increases in mitochondrial biogenesis as well. This correlation may be related to how PDE5 inhibition leads to skeletal muscle hypertrophy.
PDE5 inhibitors also seem to increase cyclic adenosine monophosphate (cAMP) levels at an even greater magnitude than it increases cGMP, according to one study [8]. There is quite of body of evidence to suggest that elevation of cAMP leads to hypertrophic responses, so this piece of data is extremely compelling in the argument at hand. Quoting one study in particular [9], "Strikingly, sustained activation of cAMP signaling leads to pronounced hypertrophic responses in skeletal myofibers through largely elusive molecular mechanisms".
In human osteoblast cells (in vitro), tadalafil has also been shown to increase androgen receptor (AR) content while simultaneously decreasing aromatase (ARO) content [10]. Since androgens (testosterone, DHT, and even exogenous anabolic steroids) play a very large role in mediating hypertrophy, it is completely plausible to say that this upregulation of ARs would lead to increases in overall hypertrophy. Aromatase is responsible for "breaking down" some androgens, so a decrease an ARO both logically and in literature may lead to an increase in hypertrophy as well. The only caveat to this would be the magnitude at which ARO is decreased, as very low estrogen levels decrease anabolic response in humans, which may offset the increase in hypertrophy via AR upregulation altogether.
Possible Contradictions
There is one moderately significant study with data that contradicts the aforementioned points [11]. This study was pointed out by TNF in his response to my video (you can watch it here). In this study, there were four groups of rodents: sedentary (n=5), sedentary + sildenafil (n=5), trained (n=10), and trained + sildenafil (n=10). Although this study does show a decrease of skeletal muscle hypertrophy in mice in the trained + sildenafil group versus the trained group, there are a few problems with it:
- These rodents were running on a wheel - they were not doing resistance training
- Some data from this study contradicts other studies
- The deduction from this data that sildenafil decreases hypertrophy itself is conflicting
Point one is pretty self-explanatory. One could make the argument that if PDE5 inhibitors do illicit hypertrophic responses, they should do so regardless of the circumstance, but the mechanism of PDE5 inhibitors increasing hypertrophy is so elusive with the current evidence that we're not exactly sure if that would hold up practically.
As for point two, the data regarding PRC-1a (involved in mitochondrial biogenesis) expression entirely contradicts multiple studies cited previously. In this study, PRC-1a expression was decreased following sildenafil administration, but multiple other studies show the opposite.
Finally, making the deduction from this evidence that sildenafil decreases hypertrophy just doesn't make sense if you look at all of the data. FoxO3a, a protein responsible for regulating muscle atrophy, did not change significantly in skeletal muscle myonuclei between the two groups of sedentary rats, but only in the two groups of trained rats. This would suggest that the training style of the rodents may have potentiated the atrophy, not the sildenafil itself.
Nonetheless, this study is one of the few that poses a decent rebuttal to the rest of the evidence we have.
Conclusions and Deductions
In my opinion, there is a large bit of compelling evidence showing that PDE5 inhibitors do increase skeletal muscle hypertrophy. All things considered, the evidence in favor of PDE5 inhibitors increasing muscle hypertrophy vastly overshadows the evidence of the contrary.
Sources:
[1] Monique Curran & Gillian Keating (2003), "Tadalafil"
[2] Melinda Sheffield-Moore Ph.D et al. (2013) "Sildenafil Increases Muscle Protein Synthesis and Reduces Muscle Fatigue"
[3] Akihiro Asai , Nita Sahani, Masao Kaneki, Yasuyoshi Ouchi, J. A. Jeevendra Martyn & Shingo Egusa Yasuhara (2007), "Primary role of functional ischemia, quantitative evidence for the two-hit mechanism, and phosphodiesterase-5 inhibitor therapy in mouse muscular dystrophy"
[4] Justin M Percival , Nicholas P. Whitehead, Marvin E. Adams, Candace M. Adamo, Joseph A. Beavo & Stanley C. Froehner (2012) "Sildenafil reduces respiratory muscle weakness and fibrosis in the mdx mouse model of Duchenne muscular dystrophy"
[5] Enzo Nisoli et al. (2003), "Mitochondrial biogenesis in mammals: the role of endogenous nitric oxide"
[6] Kim S. Lau, Robert W. Grange, Wen-Jinn Chang, Kristine E. Kamm, Ingrid Sarelius, & James T. Stull (1998), "Skeletal muscle contractions stimulate cGMP formation and attenuate vascular smooth muscle myosin phosphorylation via nitric oxide"
[7] Arsalan Damirchi, Parvin Babaei, Meysam Gholamali & Kamal Ranjbar (2012) "Mitochondrial Biogenesis in Skeletal Muscle: Exercise and Aging"
[8] Daniel G. Corum et al. (2020), "PDE5 inhibition rescues mitochondrial dysfunction and angiogenic responses induced by Akt3 inhibition by promotion of PRC expression"
[9] Rebecca Berdeaux & Randi Stewart (2012), "cAMP signaling in skeletal muscle adaptation: hypertrophy, metabolism, and regeneration"
[10] A. Aversa et al. (2016), "Tadalafil modulates aromatase activity and androgen receptor expression in a human osteoblastic cell in vitro model"
[11]